

A point of care emergency clinical summary has been created for Acute Coronary Syndromes (ACS) in women. This core document will be accompanied by additional documents/tools focusing on specific conditions that can cause MINOCA. The BC Emergency Medicine Network was our first dissemination point, with further dissemination on our horizons. The development of these women’s heart health-specific tools, including checklists and flowcharts, will support front-line decision-making.
Chest Pain in Women in the Emergency Department:
A Focus on Acute Coronary Syndrome
1. SCOPE OF THE PROBLEM:
Cardiovascular disease (CVD) is the leading cause of premature death in women in Canada1. Mortality rates in men have stabilized in the last decade but have continued to increase in women in Canada2 and can occur for women of all ages. Sex and gender-specific differences exist in awareness, symptom presentation, diagnosis, prognosis, and treatment3. The diagnosis of acute coronary syndrome (ACS) in women presenting to the ER can be complex and challenging. Rapid diagnosis and treatment are vital.
2. SYMPTOMS:
More than 50% of women who experience heart attacks have their symptoms unrecognized by healthcare providers4. In addition, women are 7x more likely to be sent home5. Chest discomfort is the most common presenting complaint in 90% of ACS, in BOTH men and women4. Women may, however, describe their symptoms differently than men, as discomfort or pressure rather than “pain.” Anginal equivalents, such as dyspnea, epigastric pain, and upper back discomfort, are more often reported in women, and may lead to misdiagnosis and delays in treatment. Heart attacks are on the rise and can occur in women of all ages. Assessing for cardiac disease should be prioritized in women who experience chest pain/pressure.

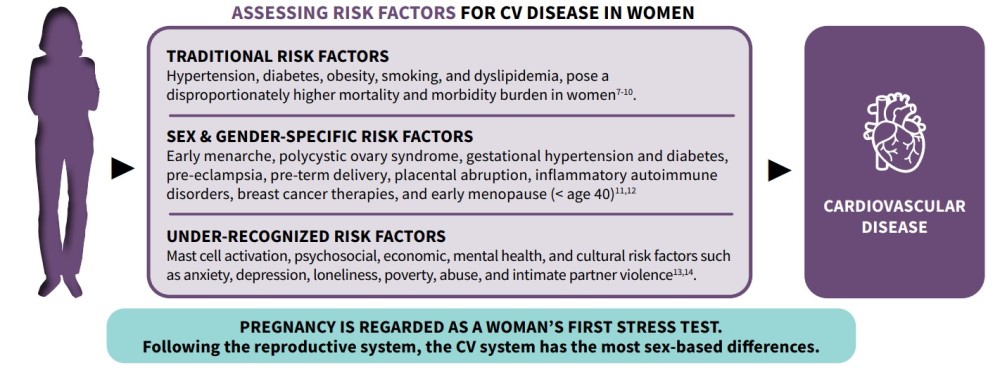
3. RISK FACTORS:
Cardiovascular risk assessment in women requires evaluation of traditional, sex-gender specific, and under-recognized risk factors6:
 <
<
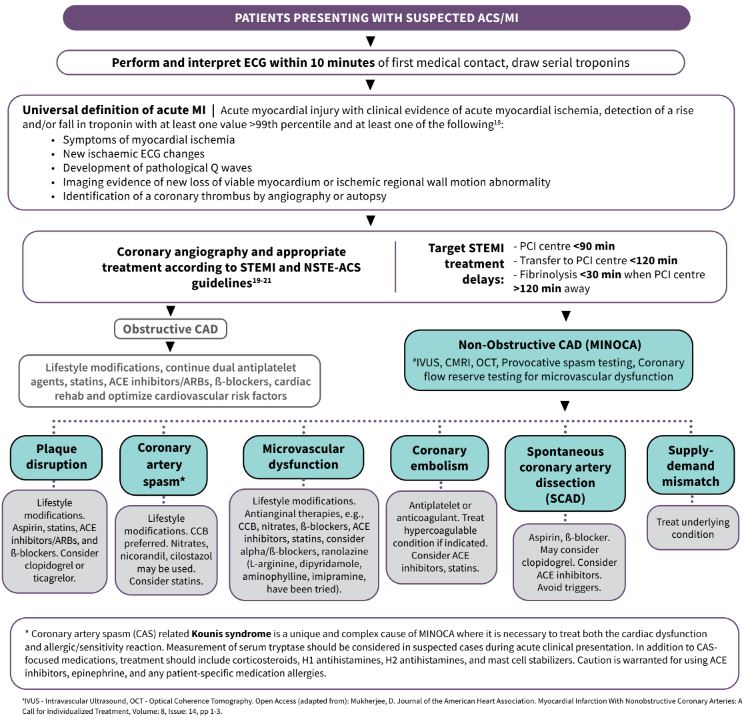
4. PATHOPHYSIOLOGY:
Coronary Artery Disease (CAD), is a type of CVD that can be obstructive or non-obstructive. Obstructive coronary artery disease (ST and non-ST elevation myocardial infarction) is common in both men and women. However, in 5-15% of ACS cases, Myocardial Infarction with Non-Obstructive Coronary Arteries (MINOCA) can occur, particularly in women15. The coronary angiogram in MINOCA reveals < 50% stenosis in any major epicardial artery. Serial troponins, preferably high-sensitivity assays, using sex-specific thresholds, are critical, as initial results may be normal. Initial troponin should be followed by repeat sample collection 1-3 hours later for high-sensitiviy troponin and 3-6 hours later for conventional troponin assays16. Long term prognosis for MINOCA patients may include worse quality of life indicators, compared to obstructive MI patients.
5. POTENTIAL CAUSES OF MINOCA:
Possible causes of MINOCA include, but are not limited to, plaque rupture/erosion, coronary artery vasospasm (including ACS syndrome accompanying mast cell activation from allergic, hypersensitivity, or anaphylactic reactions: Kounis syndrome)17, microvascular dysfunction, coronary artery embolism, and spontaneous coronary artery dissection (SCAD)15.
6. INVESTIGATIONS AND MEDICAL THERAPY:
7. DIFFERENTIAL DIAGNOSIS:
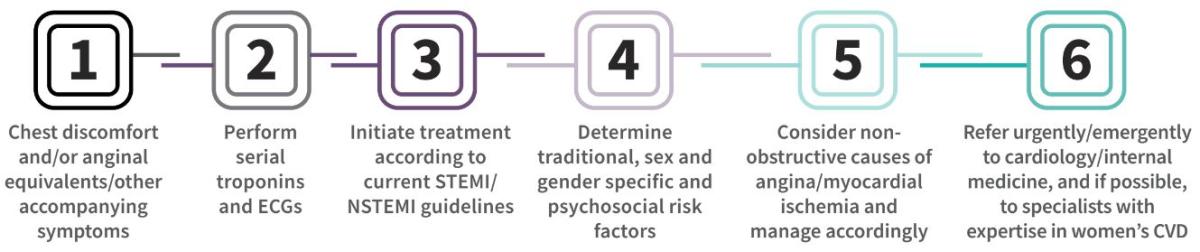
8. ACS IN WOMEN CHECKLIST:
9. ADDITIONAL RESOURCES:
- Canadian Women’s Heart Health Alliance ATLAS of the Epidemiology, Diagnosis and Management of CVD in Women
- A free and accredited Canadian Women’s Heart Health Education Course and Toolkit
10. ACKNOWLEDGEMENTS:
This educational material is brought to you by the Knowledge Translation and Mobilization Working Group (KTMWG) of the Canadian Women’s Heart Health Alliance (CWHHA). The composition team includes Dr. Shahin Jaffer, Dr. Christine Pacheco, Dr. Najah Adreak, Dr. Jill Bruneau, Helen Robert, Karen E. Jacques, and Meagan Noble. The CWHHA is powered by the Canadian Women’s Heart Health Centre at the University of Ottawa Heart Institute.
REFERENCES:
- Jaffer, S. Epidemiology, Diagnosis, and Management of Cardiovascular Disease in Women—Scope of the Problem (2020) CJC Open.
- Lopez, AD. Is the long-term decline in cardiovascular-disease mortality in high-income countries over? Evidence from national vital statistics (2019) Int J Epidemiol.
- Pacheco, C. Epidemiology, Diagnosis, and Management of Cardiovascular Disease in Women—Sex- and Gender-Unique Manifestations of Cardiovascular Disease (2021) CJC Open.
- Lichtman JH, et al. Sex Differences in the Presentation and Perception of Symptoms Among Young Patients With Myocardial Infarction: Evidence from the VIRGO Study (Variation in Recovery: Role of Gender on Outcomes of Young AMI Patients). Circulation. 2018;137(8):781-790.
- Bugiardini R, Ricci B, Cenko E, et al. SEX-RELATED DIFFERENCES IN ACUTE CORONARY CARE AMONG PATIENTS WITH MYOCARDIAL INFARCTION: THE ROLE OF PREHOSPITAL DELAY. J Am Coll Cardiol. 2015 Mar, 65 (10_Supplement) A8.
- Vogel B et al., The Lancet women and cardiovascular disease Commission: reducing the global burden by 2030, Lancet 2021 Jun 19;397(10292):2385-2438.
- Mosca, L. Effectiveness-Based Guidelines for the Prevention of Cardiovascular Disease in Women—2011 Update: A Guideline From the American Heart Association (2011) JACC.
- Steptoe, A. Stress and cardiovascular disease (2012) Nat Re Cardiol.
- Cohen, BE. State of the Art Review: Depression, Stress, Anxiety, and Cardiovascular Disease (2015) American J Hypertension.
- Garcia, M. Cardiovascular Disease in Women: Clinical Perspectives (2016) Cir Res.
- Mehta, L S. Acute Myocardial Infarction in Women: A Scientific Statement From the American Heart Association (2016) Circulation.
- Norris, C M. State of the Science in Women’s Cardiovascular Disease: A Canadian Perspective on the Influence of Sex and Gender (2020) JAHA.
- Coutinho, T. Hypertensive Disorders of Pregnancy and Cardiovascular Diseases: Current Knowledge and Future Directions (2018) Curr Treat Options Cardiovasc Med.
- Aggarwal, N R. Sex Differences in Ischemic Heart Disease (2018) Circulation.
- Tamis-Holland, JE. Contemporary Diagnosis and Management of Patients With Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement From the American Heart Association (2019) Circulation.
- Gulati, M. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/ American Heart Association Joint Committee on Clinical Practice Guidelines (2021) Circulation.
- Kounis, Nicholas G. Kounis syndrome: an update on epidemiology, pathogenesis, diagnosis and therapeutic management (2016) Clinical Chemistry and Laboratory Medicine.
- Thygesen, K. et al. Fourth Universal Definition of Myocardial Infarction (2018), J Am Coll Cardiol. 72 (18) 2231–2264).
- Wong, G.C. Armstrong, P.W. et al. (2019) Canadian Cardiovascular Society/Canadian Association of Interventional Cardiology Guidelines on the Acute Management of ST-Elevation Myocardial Infarction: Focused Update on Regionalization and Reperfusion. CJC V35, Issue 2; 107-132.
- Collet et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC) (2021) Eur Heart J.
- Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;64:e139-e228.